Email us:
info@andrea-digestive-clinic.comCall us:
+65 6264-2836#21-11/12 Royal Square Medical Centre
Mon - Fri : 9am - 5pm, Sat : 9am - 1pm

Colorectal cancer (CRC) or colon cancer for short, represents the third most common cancer worldwide, with about 1.8 million new cases in 2018. It is the most common cancer in Singapore with approximately 1200 new cases diagnosed each year. Recently, increase in CRC in younger adults was reported the United States and few other developed countries, according to study analysis published in GUT in September 2019. CRC incidence increased in young adults (20-34 years old), which is potentially signalling changes in early-life exposures that influence large bowel carcinogenesis.
Commonly known risk factors for developing CRC are older age, male gender, family history, smoking, processed meat consumption and obesity. Behavioural factors, such as obesity and physical inactivity, may also play a role. The prevalence of obesity has risen in the United States, and that is a known contributor to CRC, along with physical inactivity. The diet high in red meat, junk food, and processed meats and low in fresh vegetables has been associated with an increased risk for colon cancer.

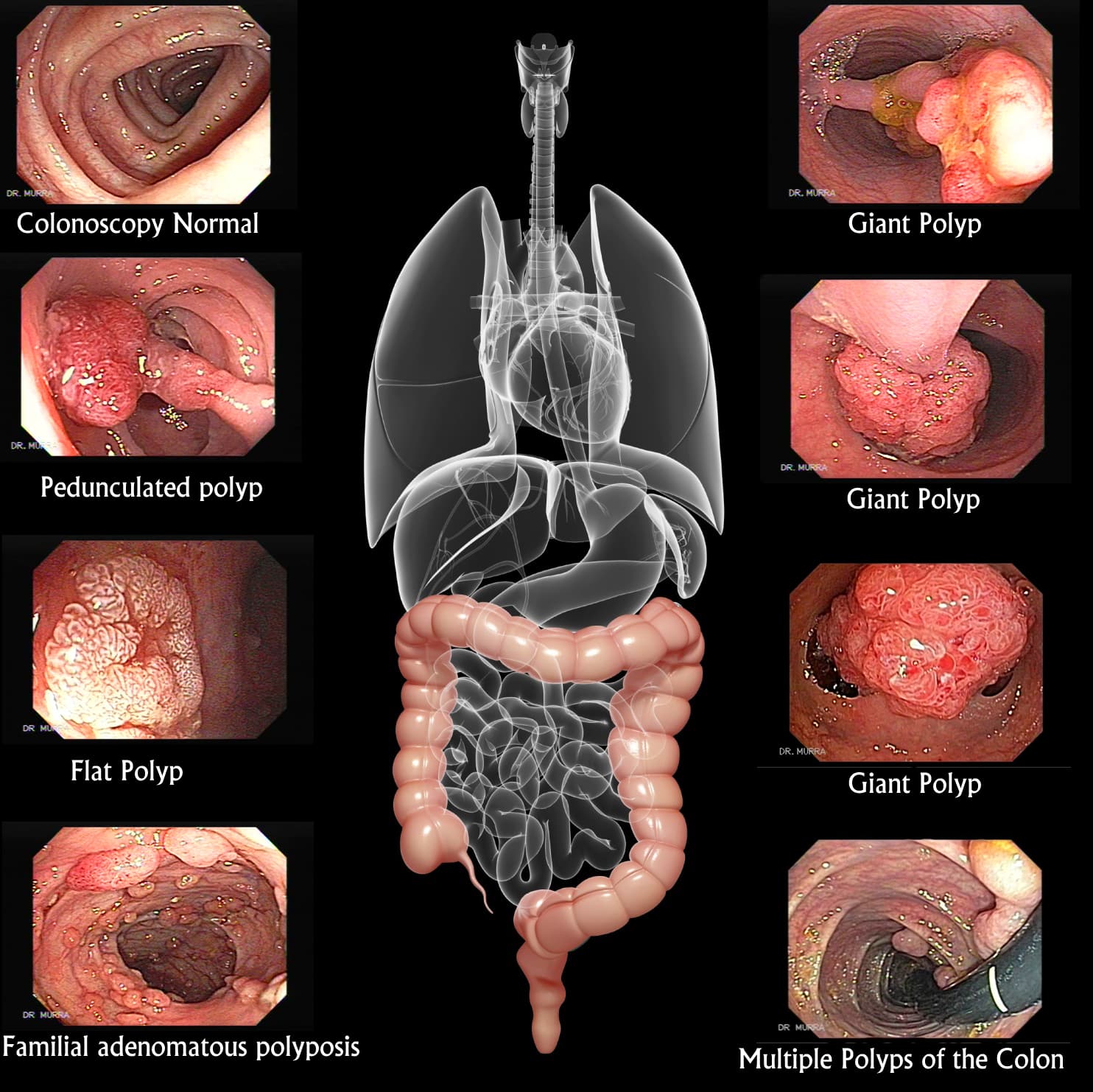
The majority of colorectal cancers arise from adenomatous polyps. Adenomatous polyps are largely asymptomatic. The process of malignant transformation takes a relatively long time. Malignant transformation of adenomatous polyps (adenoma-carcinoma sequence) takes 5 to 10 years via multiple gene mutations. Adenomatous polyps are relatively asymptomatic. They are present in up to 25% of individuals at age 50 and the prevalence increases with age. Most polyps (90%) can be removed at colonoscopy, thereby precluding the need for surgery.
Thus, colorectal cancer has a detectable premalignant phase (adenoma) and a relatively long duration of malignant transformation. Mortality from colorectal cancer can be reduced by screening asymptomatic individuals for the presence of adenomas and early cancers. CRC screening can help to detect and remove pre-malignant lesions, such as colonic adenoma, or diagnose early asymptomatic cancer to improve outcomes.
Many patients with CRC are diagnosed at Stage III or later, which is associated with poor survival. At this stage, patient may experience several of these symptoms: change in bowel habit, including constipation or diarrhea and their combination, change in the stool consistency, incomplete bowel evacuation, rectal bleeding or presence of blood in stool, abdominal discomfort or abdominal pain, weight loss, anemia (low blood haemoglobin), tiredness, iron deficiency
Colorectal cancer (CRC) screening is the process of detecting early-stage CRCs and precancerous lesions in asymptomatic people with no prior history of cancer or precancerous lesions. Colonoscopy is considered the gold standard of colorectal cancer screening methods for its ability to view the entire colon and both detect and remove polyps during the same procedure. It is the only test that is suitable for individuals who have risk factors such as family history of CRC.
Various screening tests for colorectal cancer have been reported. Annual faecal occult blood testing (FOBT), barium enema, sigmoidoscopy and CT colonography (virtual colonoscopy). However, current evidence suggests that these alternatives may not be as effective and reliable as annual FOBT or colonoscopy in large-scale population screening.

1. Average risk – asymptomatic or family history limited to non-first degree relatives – onset at age of 50 years – repeat every 5-10 years if initial colonoscopy was normal.
2. High risk – Colorectal cancer in the first-degree relative age 60 years or younger or two or more first-degree relatives – 10 years prior to the youngest case in the family or age 40 years, whichever is earlier – repeat every 5 years
3. Personal history of colorectal polyps – repeat colonoscopy 1 to 3 years after polypectomy depends on size, number and histology of the polyps
4. Personal history of inflammatory bowel disease, ovarian, endometrial or breast cancer
5. A family history of familial adenomatous polyposis – colonoscopy or sigmoidoscopy and consider genetic counselling and testing – start at age of 10 to 12 years (from puberty)
6. A family history of hereditary non-polyposis colorectal cancer – start colonoscopy screening at the age of 20 to 25 years – repeat colonoscopy every 1 to 2 years
Prevention is better than cure. Cutting down intake of red and processed meats, high-fat dairy products, highly refined grains and starches, and sugars and replacing them with poultry, fish and plant sources as the primary source of protein can help reduce the risk. Improving the understanding of diet and healthy lifestyle with regular exercise and prevention of obesity might add further benefit and reduce risk of colorectal cancer.
Find out more information on colon cancer and colon cancer screening at Andrea's Digestive Clinic.




